
There is a swelling over my son's groin!
Your son should be examined by a paediatrician or a paediatric surgeon. There are several different diagnoses that are possible for example, inguinal hernia, hydrocele, inguinal lymph node, or tumor. A good clinical examination suffices to reach a diagnosis. Sometimes an ultrasound is needed to diagnose the cause of the swelling.
Is an inguinal hernia dangerous?
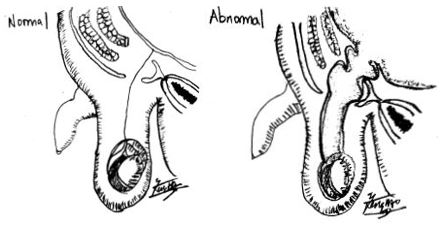
It can cause an intestinal obstruction and the risk is highest in infancy up to 30%. An inguinal hernia is a protrusion of an organ through a weakness in the tummy’s muscle wall. This is because of a patent opening and tract that extends from the tummy to the groin and to the scrotum (Figure 1). This patent tract can have a small opening which a loop of small intestine may become stuck. The blood vessels supplying the small intestine is progressively constricted as the intestine swells. In prolonged and acute obstruction, the loop of the small intestine may die because of the lack of blood supply.
Can medicines cure an inguinal hernia?
Unfortunately, no medicine can close the opening and weakness in the tummy’s muscle wall. Only surgery can repair the anatomical defect.
When is the best time to repair an inguinal hernia?
The repair of an inguinal hernia in a baby or child or teenager is time sensitive, and should be performed as soon as the baby is fit for surgery. This is because of the risk of obstruction and subsequent strangulation of intestine due to the hernia. When an inguinal hernia is perceived to be stuck, I will reduce it myself. When I can reduce it, I recommend operation within 24 to 48 hours. When I am not able to reduce it, I perform key hole (laparoscopic) hernia repair emergently because there is the risk of bowel or testicular or ovarian compromise of blood supply.
What happens during a laparoscopic / open inguinal hernia repair?
During discussion, I recommend a single site key hole (laparoscopy) procedure. The incision is concealed within the umbilicus. Laparoscopy is essential to visualize both inguinal openings. This is because up to 50% of patients have a concurrent patent opening and tract on the other side of the tummy(1). Those with a patent opening on the other side presents with a hernia in 5 to 13% of patients in the future (2). A laparoscopic hernia repair can be performed if there are bilateral hernias. The patient is put under general anaesthesia and a single keyhole incision is made to insert the laparoscopic instruments. The hernia opening(s) in the tummy is then repaired. The laparoscopic instruments are removed and the wounds are closed with absorbable stitches.
If there are reasons against a laparoscopic hernia repair, the operation can be performed via an open technique (2). The patient is put under general or regional anaesthesia. A groin skin incision is made, the hernia opening and tract are repaired. The wound is closed with absorbable stitches. Local anaesthesia is given in both techniques to ensure a painless recovery.
Both techniques are day surgeries, and the patient can go home on the same day.
How is the recovery after an inguinal hernia repair?
Minimal bleeding is expected from the wound. The patient can have normal baths. Painkillers may be required for the first 2 to 3 days. For babies, I recommend checking the diapers 2 to 3 hourly. If soiled, please change the diaper to keep the wound clean. A scab forms over the wound normally in the first 2 weeks and drops off with time. Risks of the surgery are infection, recurrent hernia, damage to the testis, and repeat surgery. Infection presents as redness, swelling, pain, warmth and abnormal discharge of the wound site(s). If any of these complications occur, treatment is available and I can be consulted early. It is important to avoid swimming and exercise for 4 weeks to allow the wound to have good healing and strength.
What is the cost of a laparoscopic inguinal hernia repair?
The total cost estimate for the laparoscopic inguinal hernia repair and a 1 bedded day surgery ward is $20,383 inclusive of GST. This is less than the cost when the same procedure is done in a private hospital similar 1 bedded ward for example Mount Elizabeth Novena Hospital of $26,733 – $33,315 (reference: https://www.moh.gov.sg/managing-expenses/bills-and-fee-benchmarks/cost-financing/tosp-sf820a-bill-information/). This includes, the surgeon fee, the anaesthetist fee, the doctor’s attendance fee, operation theatre fee, 1 bedded ambulatory surgery ward fee, standard consumables and medications used. This is a concerted effort to keep costs affordable for patients.
References
1) Staerkle RF, Guglielmetti LC, Bielicki IN, et al. Is it worth to explore the contralateral side in unilateral childhood inguinal hernia?: A PRISMA-compliant meta-analysis. Medicine (Baltimore). 2020 Jul 31;99(31):e21501.
2) Kantor N, Travis N, Wayne C, et al. Laparoscopic versus open inguinal hernia repair in children: which is the true gold-standard? A systematic review and meta-analysis. Pediatr Surg Int. 2019 Sep;35(9):1013–26.
3) Esposito C, Escolino M, Turrà F, et al. Current concepts in the management of inguinal hernia and hydrocele in pediatric patients in laparoscopic era. Semin Pediatr Surg. 2016 Aug;25(4):232–40.
Share if you like this post
If you have other enquiries on children’s surgical conditions, feel free to contact us
© Copyright- 2022 Paediatric Surgery and Urology International
All Rights Reserved